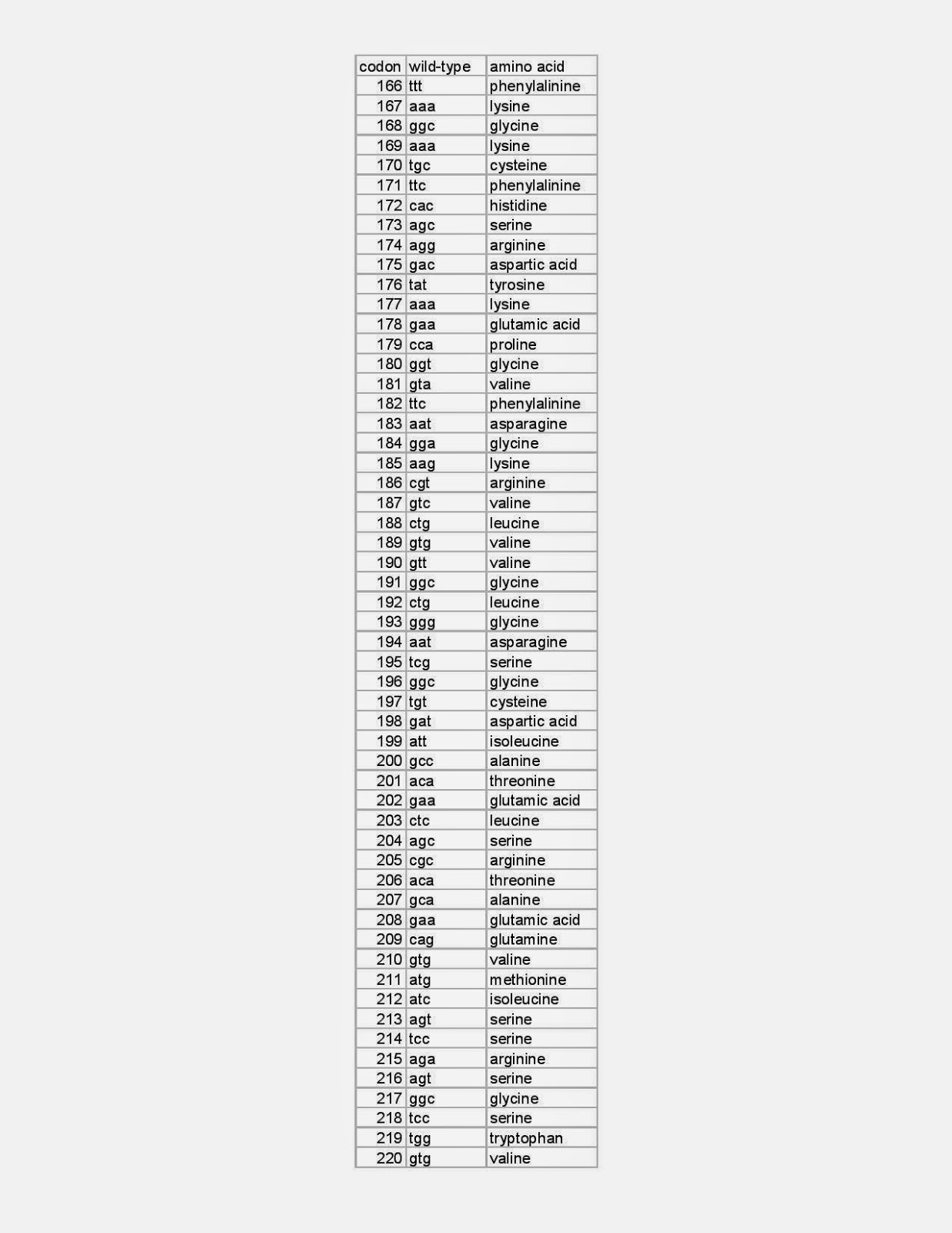
FMO3 is a 532 amino acid sequence, and 23andme only test about 50 of the 532, but it does test the 3 main variants at codons 158, 257, 308.
It would be interesting to see if most of carry 2 or more of these.
Estimates of carriers of the 3 main variants :
E158K : 40% people ?
E308G : 20% ?
V257M : 10% ?
DIY STUDY
We should be aiming to flood PUBMED with papers about TMAU, SysBO/Hali etc.
PUBMED is where researchers look to see whats going on.
But for now, as beggars, we can try a DIY STUDY.
Question
Do you carry E158K, V257M and/or E308G ?
Feel free to put your result in the COMMENT SECTION.
Anon if you want ?
e.g.
E158K : AG
V257M : AA
E308G : AG
HOW CAN I TEST FOR THIS ?
A cheap and easy way to test for the 3 most common FMO3 variants is :
1. Find and buy an ancestry test that lets you download the RAW DATA ...
or buy 23andme.com test.
2. Look for these 3 variants :
rs2266782
variant known as E158K
normal : GG
variant : A
rs1736557
variant known as V257M
normal : GG
variant : A
rs2266780
variant known as E308G
normal : AA
variant : G
FMO3 PROTEIN is a 532 amino acid sequence, but there are 3 most common variants. E158K V257M E308G . Many people carry these faults (Whites carry maximum for the 3 : 45%, 25% 10% ... estimate from memory). No-one is bothered much to find out if they are 'pathogenic' or not, but it would be interesting to see if those who identify with metabolic malodor tend to carry them in a mix.
My own current view :
I suspect most cases of 'metabolic/systemic body odor' are due to weakness in the FMO3 enzyme, but there may be other enzyme disorders too.
COMMENT SECTION
Feel free to put your result in the comment section. Anon if you want.
Get new posts by email